
Mastering the D4341 Dental Code: The Definitive 2026 Guide for Dental Practices
Dental practices today face a maze of American Dental Association CDT codes; mastering the high-volume ones is the only path to real financial health. Take the D4341 dental code. It’s arguably the most vital lever for your revenue cycle and clinical bottom line.
Get it wrong, and you’re looking at a spike in denials, stalled reimbursements, and a compliance headache you don’t need. But when you truly master the D4341 dental code description and back it up with rigorous, bulletproof documentation, the opposite happens. You slash those costly denials while delivering essential periodontal disease treatment USA patients need most.
Maybe you're an office manager hunting for a clean, compliant D4341 dental code definition. Or perhaps your billing team is looking to overhaul internal dental insurance billing workflows. Either way, this 2026 operational guide is your blueprint. It’s designed for one thing: getting you to compliant billing, administrative sanity, and maximum reimbursement.
1. What is D4341 Dental Code Used For?
To establish unassailable clinical legitimacy for your insurance submissions, it is important to understand exactly what the D4341 dental code is used for. The procedure code D4341 is a therapeutic intervention, not a preventive one. It is explicitly indicated for patients who require an intensive deep cleaning procedure to address active bone loss, attachment loss, and structural degradation of the supporting tissues.
The core of this clinical treatment relies on thorough scaling and root planing, which involves meticulous dental plaque removal and deep calculus removal from the root surfaces within a diseased periodontal pocket. Unlike routine cleanings, this dental CPT code D4341 is a foundational element of long-term periodontitis management and comprehensive gum disease treatment, aiming for complete oral health restoration.
The Clinical Mechanics of Root Instrumentation
When an administrative reviewer looks at a claim, they assess whether the clinician performed true therapeutic instrumentation. The procedure requires instrumentation of both the crown and root surfaces to eliminate supra- and subgingival plaque, calculus, and endotoxins.
It is a highly demanding clinical process designed to create a biologically acceptable surface to allow for tissue reattachment. Because of this complexity, payers scrutinize “what is a D4341 dental code” application profiles to confirm that the clinical reality justifies the specialized reimbursement rate.
2. Clinical Documentation Criteria & ADA Guidelines
Adhering to the formal ADA guidelines for D4341 requires building a systematic approach to chart notes and claim attachments. Insurance processors look for clear markers that establish medical necessity.
Mandatory Verification Elements
To ensure your claims actually satisfy major payers, your operational protocols must include these:
Full-Mouth Periodontal Charting
This needs to be current (within the last 12 months), and it has to detail pocket depths of 4mm or greater across four or more teeth in that quadrant.
Diagnostic Radiographs
You’ve got to use clear, diagnostic-quality periapical or bitewing radiographs; they must show visible alveolar bone loss, root roughness, or subgingival calculus deposits.
Detailed Clinical Narratives
Don’t hold back here; your notations must explicitly document localized bleeding on probing (BOP), soft tissue inflammation, furcation involvement, or even mobility.
“In our experience, those automated claims scrubbers big insurance companies use will routinely reject claims if you only submit a standard panoramic X-ray. It’s a mess; they don't have the detail. You’ve got to include bitewing or periapical views, because horizontal bone loss and fine subgingival calculus just can't be accurately verified on a panoramic film alone.”
3. Scaling vs Regular Cleaning: The Difference Between D4341 and D1110
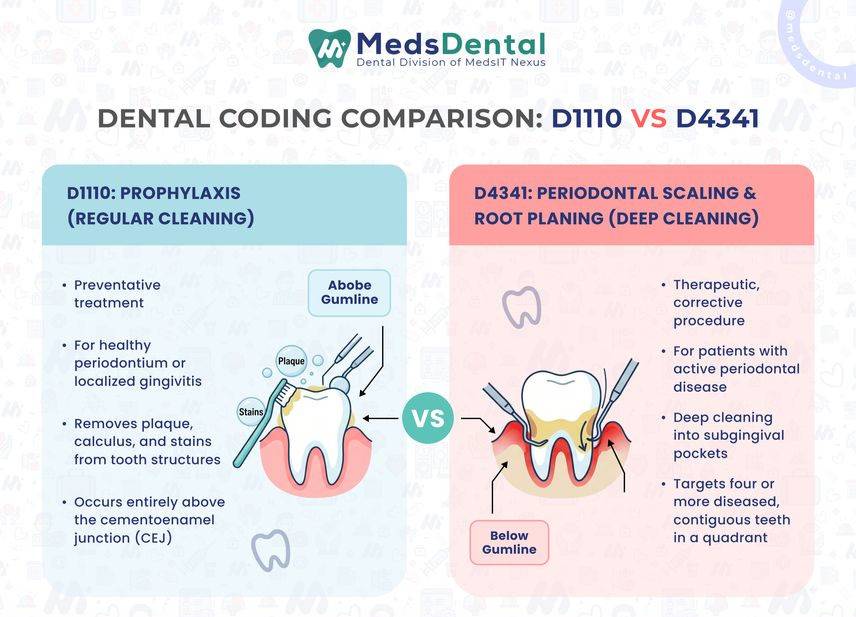
A frequent point of confusion for front-office teams and cross-trained administrative staff is distinguishing between scaling vs regular cleaning codes, specifically the difference between D4341 and D1110. Misapplying these codes is a leading trigger for external insurance audits and catastrophic balance-billing friction with your patient base.
-
D1110 (Prophylaxis): A preventative treatment performed on a healthy periodontium or a patient with localized gingivitis to remove plaque, calculus, and stains from the tooth structures. It is preventive, meaning it occurs entirely above the cementoenamel junction.
-
D4341 (Periodontal Scaling & Root Planing): A therapeutic, corrective procedure targeting four or more diseased, contiguous teeth or bounded tooth spaces within a single quadrant. It is fundamentally therapeutic, extending deep below the gumline into the subgingival pocket environment.
Coding accuracy always depends entirely on the patient's diagnostic data. If we look at the diagnostic metrics showing that only one to three teeth in a quadrant require subgingival instrumentation, your team must pivot away from D4341 and look to its sister code, D4342.
On the other hand, if your team is confused about whether a dental hygiene deep cleaning or a standard prophylaxis is required, always defer to the clinical data showing active periodontal disease to support the application of the ADA CDT D4341 designation.
Understanding whether a dental hygiene deep cleaning is clinically justified means trusting the objective data over subjective patient requests.
4. Periodontal Treatment Cost vs Cleaning
Look, I get the frustration. Patients see a bill for scaling and root planing, and they immediately compare it to their routine, "free" six-month cleaning. It’s an uphill battle at the front desk, but you’ve got to flip the script. Stop trying to justify a line item and start explaining why their gums are in trouble.
If you’re calling it a "deep cleaning," you’ve already lost the battle. Start calling it what it is: periodontal therapy.
Stop the "Compare and Contrast" Trap
When a patient asks why the price is so high, don’t just list bullet points. That sounds like a script. Instead, break down the reality of what’s happening in the chair.
Routine cleanings - the D1110s we do all day- are just maintenance. It's light plaque, surface-level polish, and a quick check-up. Easy. But D4341? That's a clinical intervention for active disease. We’re going below the gumline to manually scrape out years of calcified bacteria. We’re working on tooth roots that are essentially under attack.
It’s physically harder on the hygienist, it takes twice the time, and quite honestly, it’s a surgical-level process. We’re using local anesthesia because, frankly, you wouldn't want us digging into those inflamed, bleeding pockets without it.
Why the Price Actually Matters
Patients need to realize that every dollar they spend on SRP is a dollar they aren't spending on an implant or a bridge later on.
-
It’s specialized time. We aren't just polishing teeth; we’re debriding deep, infected pockets.
-
The technology is different. We’re using ultrasonic scalers specifically tuned to pull off hardened tartar from root surfaces.
-
The diagnostic burden is huge. Our office is spending extra time on chart notes, X-rays, and insurance narratives just to get the claim paid so the patient gets their benefit.
In our experience, If a patient skips this because of the copay, they’re going to lose their teeth. It’s that simple. When you talk to them, don’t talk about codes or quadrants. Talk about their bone. Talk about the fact that they’re currently losing the foundation of their smile. Once they realize they’re paying to keep their own teeth, the price tag suddenly stops being the main focus.
5. Navigating the D4341 Dental Code Cost & Insurance Reimbursement
The front desk staff deals with this all day: explaining why deep cleaning isn't just a regular cleaning. It costs more. Patients get it, or they try to, but they always ask the same thing: "What's the price on this?" They hate seeing a higher out-of-pocket cost than a normal checkup. I get it.
Prices for the D4341 CPT code? They aren't fixed. Anywhere from $200 up to $450 per quadrant is standard in the States. Depends on your location, how fancy the office is, and who the doctor is.
My advice for the desk: stop talking about the fee. Start talking about the patient's teeth. Tell them: this is an investment in your bone, and it's called a deep cleaning dental procedure USA. We are stopping the tissue breakdown. If you skip this, your long-term health pays the price. Massive dental bills? That's what you're avoiding. Keep the focus there.
Insurance Coverage Realities
Most major dental insurance providers (Delta Dental, Aetna, Cigna) offer coverage for this procedure, but they scrutinize the SRP cost with insurance USA closely to protect their loss ratios. To streamline your periodontal therapy billing and maximize D4341 insurance coverage USA, your team must submit accurate documentation on the initial attempt.
Payers will analyze the provider's overall periodontal scaling cost USA and root planing procedure cost metrics against their strict regional allowances before issuing payment.
|
Code / Attribute |
D4341 (Scaling & Root Planing) |
D1110 (Prophylaxis) |
|
Type of Care |
Therapeutic / Corrective |
Preventative |
|
Target Area |
Subgingival root surfaces (4mm+ pockets) |
Supragingival tooth crowns |
|
Clinical Driver |
Active Periodontitis & Alveolar Bone Loss |
Healthy Periodontium or General Gingivitis |
|
Billing Frequency |
Subject to strict frequency limitations (e.g., once every 24-36 months) |
Typically every 6 months |
|
Insurance Coverage |
Requires objective clinical proof (Radiographs/Charting) |
Standard preventative benefit covered at 100% |
6. The B2B Path to Revenue Cycle Optimization
For a dental practice running at peak efficiency, managing deep cleaning dental procedures requires a clear division of labor between clinical staff and billing specialists. Denials frequently occur when the administrative staff files a claim under the assumption that a quadrant was treated, but the clinician's notes indicate that only three teeth met the requirements.
Developing an Internal Pre-Scrubbing Protocol
Before that D4341 claim even touches the clearing house, stop. Run it through this quick three-step filter. It’ll save you a headache later.
First: Count the teeth. Do you actually have four or more teeth in that quadrant showing clear bone or tissue loss? Don’t just assume. Look at the chart. If the math isn't there, the code won't fly.
Second: Look at your X-rays. Are those bitewings or periapicals clear? If you can’t see the bone loss or the calculus clearly, don't waste your time attaching them. It’s a guaranteed denial. Clear images or nothing.
Third: Check your dates. Is your perio chart fresh? If it’s older than a year, it’s basically worthless to the insurance company. Make sure the dates line up with the procedure before you file.
If your in-house billing team is overwhelmed by managing these multi-layered verifications alongside patient care, partnering with a dedicated dental billing company can eliminate this operational strain. Outsourcing ensures that every instance of dental procedure code D4341 usage is reviewed by certified dental coders who understand the shifting landscape of carrier policies.
7. Eliminating Coding Friction and Audit Risks
A clean revenue cycle? It all comes down to one thing: perfect alignment between your clinical documentation and your CDT code cross-references, especially those D4341 / D4341 CDT code description parameters used during tricky, multi-disciplinary medical-dental billing. Think about those cases where you bill medical insurance for patients dealing with systemic issues like pregnancy or uncontrolled diabetes. If you don't know exactly how to map that code to the medical equivalent, you’re just inviting a denial.
Don't overcomplicate it. Just stick strictly to the American Dental Association CDT codes, get your staff fully trained on the precise what is dental code D4341 metrics, and stay obsessed with objective diagnostic data. Do that, and you’ll actually mitigate denials and maximize reimbursement. Most importantly, it keeps your focus where it really belongs: delivering outstanding clinical patient care to your people.
Partner with Meds Dental To Maximize Revenue
When the nitty-gritty details of periodontal coding start slowing your practice down, Meds Dental is here to clear the path. We aren't just another outside service; we function as a seamless extension of your own team. From digging into your clinical charts to staying on top of the ever-changing, carrier-specific rules for perio claims, our experts are dedicated to keeping your revenue cycle running smoothly.
We’ll take the heavy lifting of insurance reimbursement off your plate so you can get back to what matters most, taking great care of your patients. Let us deal with the billing headaches while you focus on the chairside work.
Frequently Asked Questions
1. What is the D4341 dental code?
It’s a specific administrative medical billing identifier. Found in the CDT code classification system. It refers to periodontal scaling and root planing. We use it strictly when treating four or more diseased teeth or bounded tooth spaces within a single quadrant.
2. Is scaling and root planing necessary?
Yes. Clinically necessary? Absolutely. If a patient shows active periodontitis, bone loss, or pocket depths of 4mm or deeper, we have to act. It’s the only way to eliminate subgingival bacteria. You have to arrest the gum disease progression. It’s the primary way to prevent tooth loss.
3. How much does SRP cost in the USA?
Usually? Between $200 and $450 per quadrant. That gum disease cleaning cost varies. A lot. It depends on your geographic location. Your practice overhead. Specific provider networks.
4. Is D4341 covered by insurance?
Yes. Most commercial plans provide explicit dental deep cleaning insurance benefits. Reimbursement, however, is contingent. You have to submit proof of active disease. This means sending in recent periodontal chartings showing pocket depths of 4mm or greater and clear radiographs displaying bone loss.
5. What is the difference between deep cleaning and regular cleaning?
Depth. That’s the difference. Regular cleaning? It focuses entirely above the gumline. A healthy mouth. Deep cleaning? It targets infection beneath the gumline. It’s about arresting aggressive gum disease stages.
6. When is D4341 required?
Clinical attachment loss. That’s the trigger. Plus bone loss on X-rays. Plus pocket depths measuring 4mm or deeper. Across four or more teeth in a single quadrant.
7. How long does scaling and root planing take?
45 to 60 minutes. That’s for a single quadrant using dedicated SRP dental treatment protocols. It depends on calculus density. And, of course, patient comfort.
8. What is scaling and root planing?
Honestly, scaling and root planing is a non-surgical deep cleaning procedure. In this procedure, your dental doctors remove plaque and tartar from above and below your gum line and make your tooth roots smooth to help gums attach to the teeth.
9. What is the D4341 dental code cost in USA?
The average price for the D4341 dental code cost in USA clinics usually falls between $185 and $444 per quadrant, though this can shift based on where you live and which dentist you visit.
10. What are the benefits of deep cleaning teeth?
When it comes to the benefits of deep cleaning teeth, the main goal is to clear out stubborn plaque and tartar hiding below your gum line, which effectively halts gum disease in its tracks and brings down painful inflammation.

.jpg)